


Vaccine-Triggered Psoriasis: Unraveling the Root Cause and Path to Healing
How a Single Shot Disrupted a Young Woman’s Skin and What Science Says About Curing It


On December 31, 2020, a healthy 25-year-old woman from Arizona1 rolled up her sleeve to receive her first dose of the Moderna COVID-19 vaccine. She had no known allergies, no chronic illness, no autoimmune history. Just a typical young adult, doing what millions were doing that week — participating in a global mass vaccination campaign.
The next day, everything changed.
She was suddenly hit with a high fever, body aches, and a painful headache that confined her to bed. She missed three days of work. And then came the rash. A full-body, itchy, spreading eruption that refused to go away. By the time she saw her doctor on January 16, the inflammation had worsened, migrating across her skin in angry patches. Her physician’s verdict? New-onset psoriasis — and in other places, eczema.
“I have never had either in my life,” she told her doctor. “And I’m not allergic to anything.”
She was prescribed a prednisone injection and topical creams. But what stood out wasn’t just the diagnosis — it was the warning:
“The vaccine may have triggered an autoimmune disorder,” her doctor said. “This may go away... or you may have it for life.”
At least she was advised not to get the second dose…
If you or one of your loved ones suffer from Psoriasis, you might be interested in reading this article describing the pathological process of Psoriasis along with the ways to alleviate and cure vaccine-induced Psoriasis.
As a reminder, my commitment to helping others has put my family in dire straits. Any contribution can be helpful. So please don’t hesitate to help my family.
For those of you who read last week’s article on Eczema, you will notice that this young woman had both Eczema and Psoriasis symptoms.
They share the same trigger:
T-cell concentrated attacks on blood vessel walls
- contaminated by vaccine particles - have stripped the capillary linings and created leaks to the blood-tissue barrier in the skin capillaries.
For the record, beyond vaccines, it’s possible that localized skin infections would trigger similar phenomena, but likely on smaller surfaces.
In Eczema, skin capillaries are repaired unevenly, and small blood elements leak in.

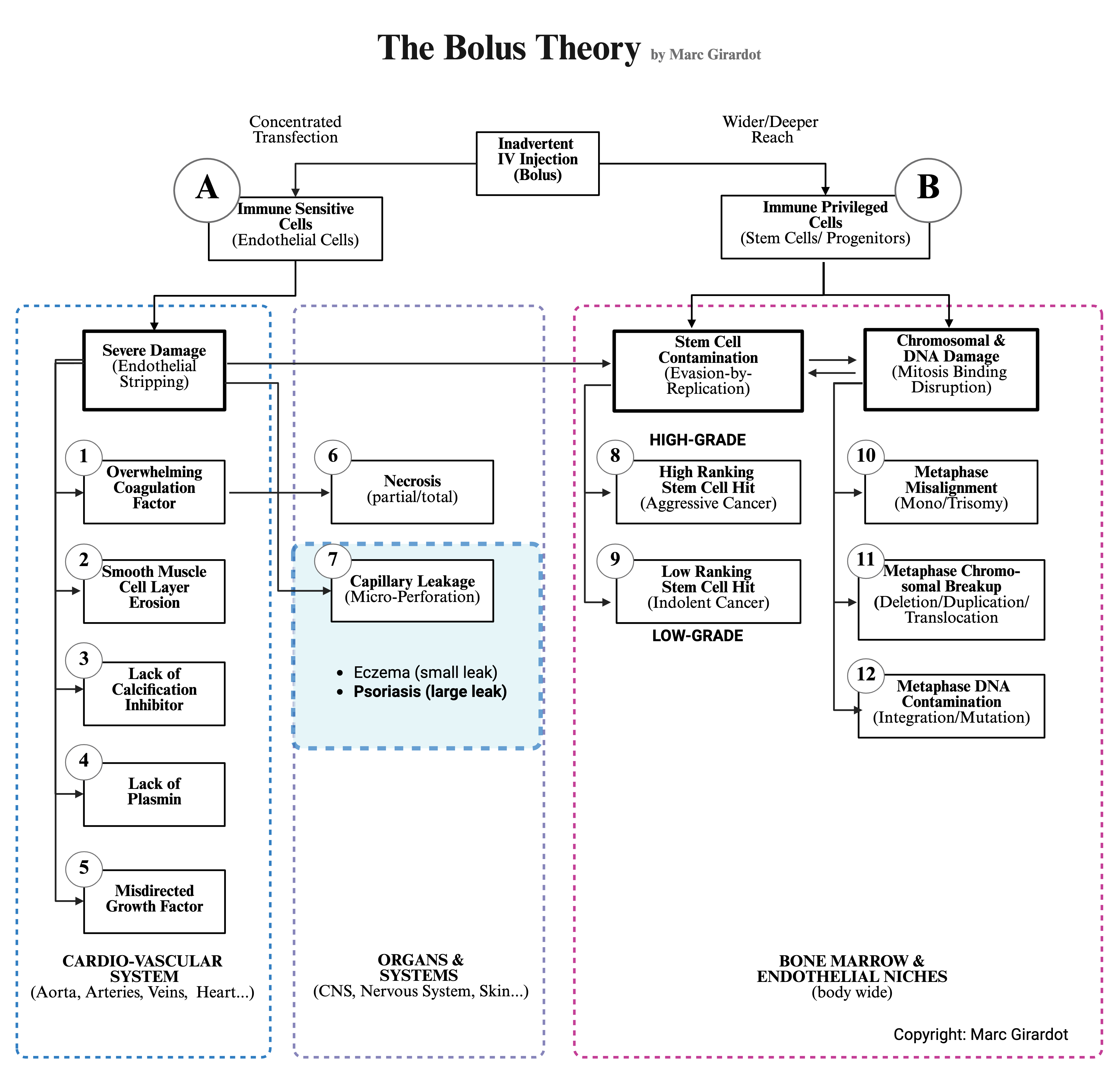
In the case of Psoriasis, the leak is wider. Larger blood elements - such as red blood cells and immune cells - constantly penetrate the skin tissue. Overall, more elements from the blood will also enter the tissue creating inflammation and triggering aberrant instances.
The two illnesses are simply different manifestations of the same destruction of the endothelial lining, possibly with differences in repair capacity. This is why this young woman from Arizona had both Eczema and Psoriaris, simultaneously.
It’s like damage after hail, some areas of the roof have tiny leaks, and some others are more seriously damaged leaking heavily. Two different outcomes tied to the severity of the damage.
The bolus of vaccine particles carpet-bombs the area and arteries upstream. Some areas are repaired evenly, some areas are repaired unevenly, and other areas aren’t repaired at all, or leave large gaps in the endothelium.
It’s very likely that Psoriasis emerges when repair is monopolized upstream, and that the repair is absent, or insufficient.
What does this larger leak in the blood-tissue barrier entail for skin tissue?
More infections
Skin tissue is normally tightly isolated from the blood, notably to avoid microbes penetrating the bloodstream and becoming systemic2. Such dysregulation would inevitably trigger many more infections, especially given the fact that the skin is not impermeable to outside contaminants. If both the epidermis (because of immature keratonicytes) and the blood-tissue barrier are no longer tight and impermeable, then any microbes can get a free pass to the entire body, and indeed people suffering from Psoriasis are 21% more subject to serious infections3.
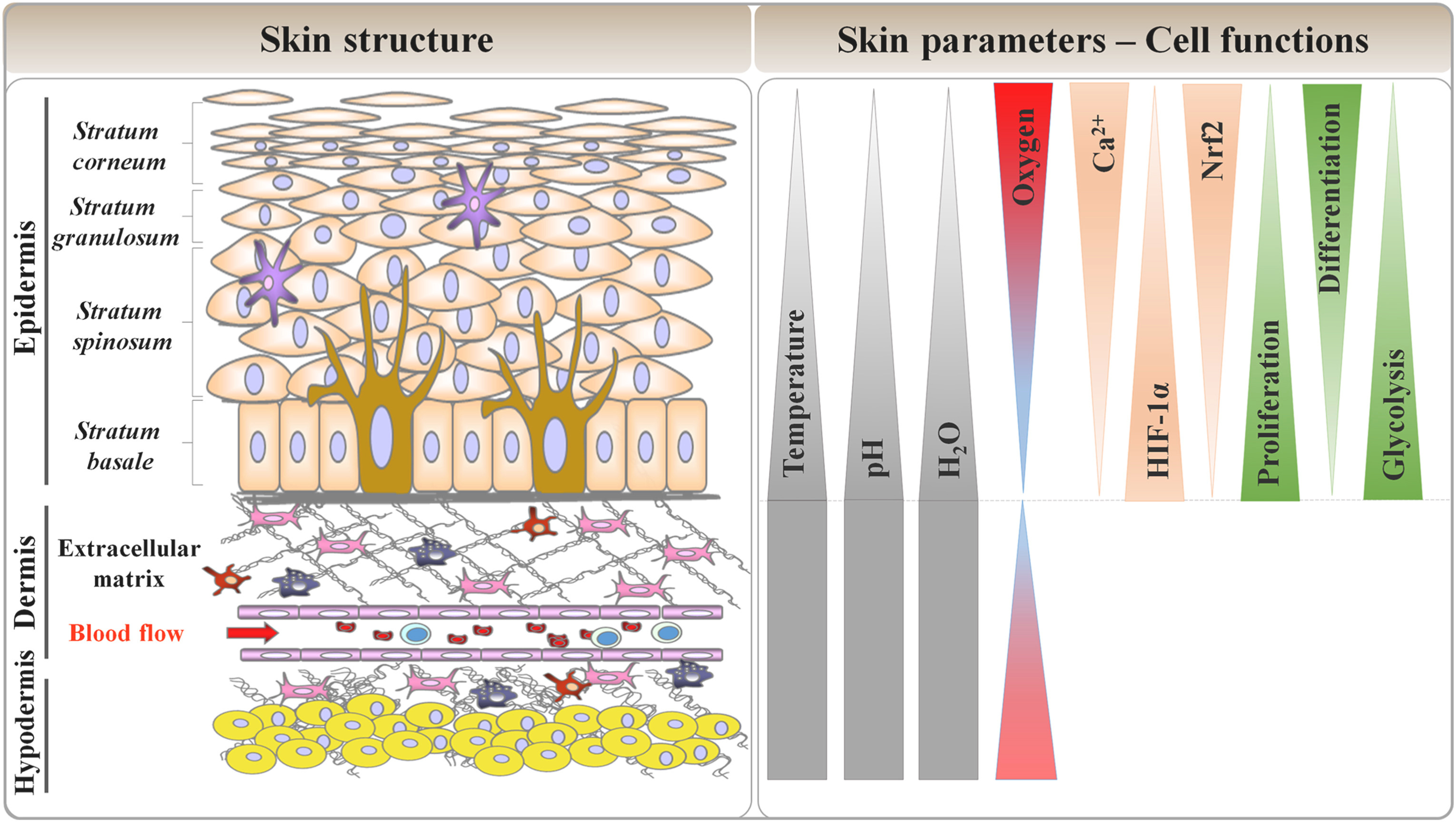
Excess Oxygen Near the Base
Contrary to many other tissues, skin tissue is under-oxygenated: 1-3% in the epidermis, and 3-7% in the dermis45. This reality means that the blood-tissue barrier in that area limits the oxygen intake.
That reality shouldn’t surprise us because the skin is dense in stem cells, and stem cells are very sensitive to oxygen. Oxygen is substituted by sugar. Glycolysis is typical of stem cells.
Loss of epidermis permeability, a normal sign of epidermis wear and need for regeneration - would inevitably let in more outside oxygen and trigger keratinocyte stem cell replication and differentiation6, a natural phenomenon to regenerate and rebuild the epidermis, in a permanent cycle of wear-and-repair.
A large leak in the capillaries would augment abnormally the oxygen level in the dermis and epidermis, as once again the filtrating function of the blood-tissue barrier is down.
Too much oxygen in the tissue at the base would abnormally stimulate keratinocyte stem cells. Hyperoxia, the over-supply of oxygen, the same process used to heal with HyperBaric Oxygen Therapy (HBOT), in this context, would stimulate local stem cells to avoid oxygen poisoning (ROS) and replicate. In other words, an abnormal amount of keratinocytes would be provisioned locally. This explains why scientists find “immature” keratinocytes in Psoriasis because the stem cells would be producing too many keratinocytes.
Everywhere the dermis capillaries are leaking significantly, hyperproliferation of keratynocytes inevitably happens, disrupting the skin ecosystem balance.

Pardon the technicalities, but it is important to understand the root cause of Psoriasis to be able to cure it.
To stop this imbalance, it is indispensable to rebuild a tight blood-tissue barrier that stops the oxygen from penetrating into the tissue and provides a stable environment for stem cells to come back to their regenerative role of maintaining the skin.
Whatever therapy is used the objective is to stimulate endothelial stem cells circulation. These stem cells will roam the body for areas to repair. When the endothelial damage is too large, only these stem cells can appropriately rebuild the blood-tissue barrier.
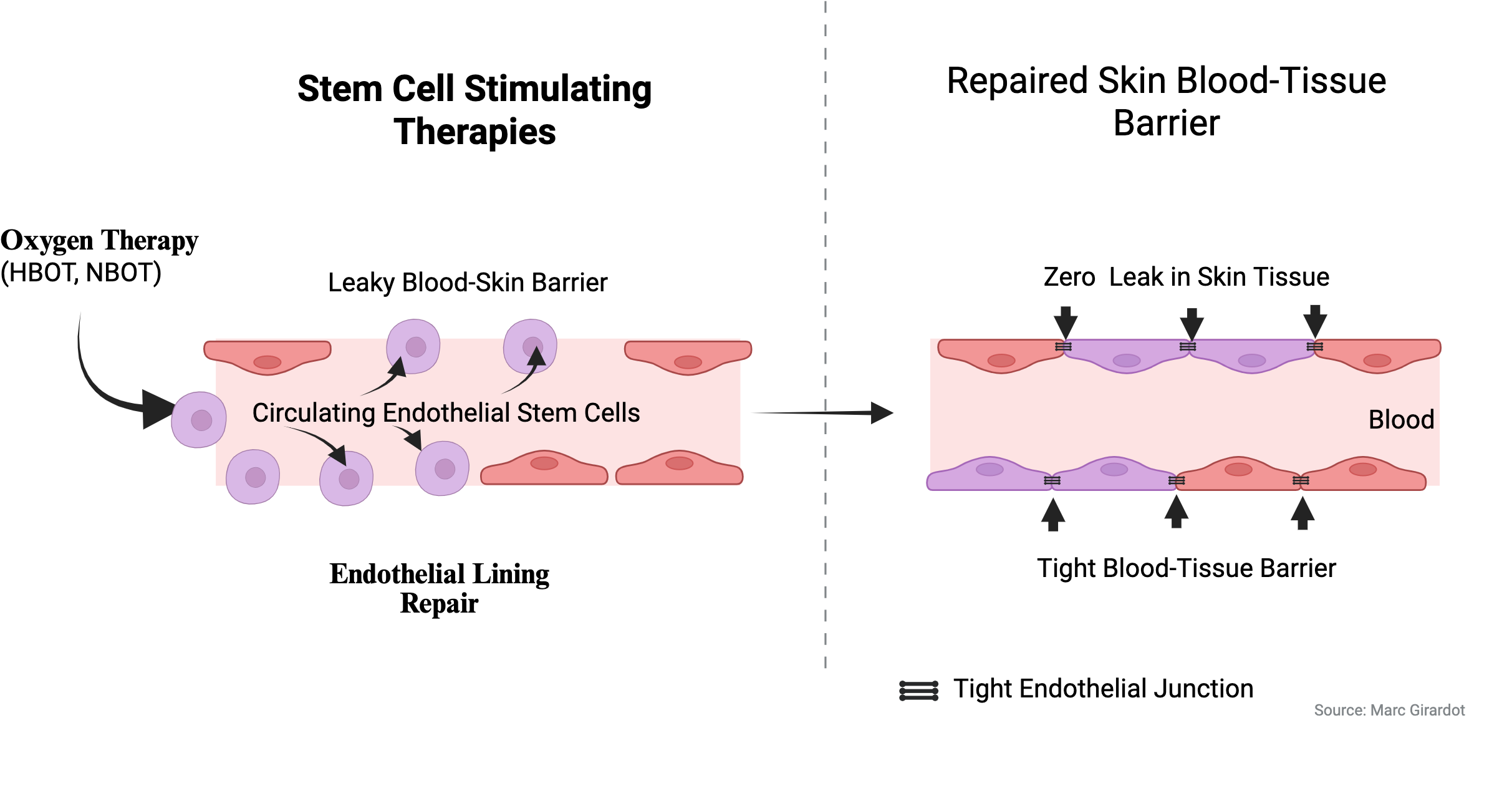
I have multiple times mentioned that endothelial healing can be achieved with oxygen therapies, either using HBOT or simply using an oxygen concentrator at home.
Unsurprisingly, two patients7 were treated with 100% oxygen, respectively at 2.8 atmospheres during 8 hours (8 x 60min sessions) and at 2 atmospheres during 22 1/2 hours (15 x 90 minutes), and obtained some excellent results.

With 95 liters diluted in the blood to stimulate stem cells, Patient 1 improved significantly, but wasn’t fully cured. By my estimate, he did roughly 1/4rth of the way to full recovery (my benchmark is 400 liters, 40 hours) .
Patient 2, with 268 liters diluted, improved greatly as he was 2/3rd of the way.
There are multiple ways to stimulate stem cells (hormetic medicine): chlorine dioxide, cryotherapy, DMSO, fasting, ivermectin, methylene blue, nicotine, red light therapy, thermotherapy, vibrations… The principle is always the same.
Oxygen therapy is so far the safest and the therapy with most replicability. I will do my best, in the coming months to try and assess the power and safety of these alternative therapies.
In any case, normobaric oxygen therapy at home with an O2 concentrator is a very affordable therapy, and more and more are sharing the benefits they are getting.
I hope you enjoyed this short article, and that it will be helpful for you or your loved ones. Please share the word, again and again. This is a very difficult disease that is curable. We need to get the word out.
I will be moving out next month. Please share this Substack. Share my book. If anyone has ways to help me professionally or financially or to help the Bolus Theory gain traction, I’d appreciate the help wholeheartedly. These are difficult times.
Love, Marc

My identifier on PayPal is marc.girardot@icloud.com
https://medalerts.org/vaersdb/findfield.php?IDNUMBER=956177
“Roles of Infection in Psoriasis” by Shihui Zhou and Zhirong Yao
“Risk of serious infection and infection mortality in patients with psoriasis: A nationwide cohort study using the Taiwan National Health Insurance claims database” by Chen et al - Reference
“Physiological skin oxygen levels: An important criterion for skin cell functionality and therapeutic approaches” by Chettouh-Hammas et Grillon - Reference
Two Pfizer shots triggered psoriasis in my healthy 60yo uncle in 2021. About a year later he received a “booster.” Three months later he was dead. There was nothing else to blame it on. Doctor even admitted it had to have been shot number three. Left behind two young adult children and his wife. The family dismisses it as a very rare unfortunate case. This isn’t the only case I could share, but it is the worst and most blatant in my family. Rest in peace, Uncle Dan.
I look forward to hearing about more solutions for psoriasis. Right now, expensive biologics are the only meds that work well but I understand there could be long term consequences of using those medicines (like all meds). The HBOT seems less risky. Thanks for writing about this subject!