


Lifting the Fog over Decades of Injuries
Vaccine Safety Myths - Mistakenly scapegoating the “circulating spike protein” would be like sweeping all the harm and pain from prior vaccine accidents under the carpet.

As many of you know, my research and investigations have demonstrated that accidental intravascular injections combined with the creation of a Bolus (a concentration of vaccine particle in the blood) via a vigorous push on the seringue plunger are likely the cause of the obscene number of vaccination accidents we have witnessed these past two years.
Many of my good friends, also fighting against what appears to be one of the worst public health decisions in history, have a different perspective and believe it is the circulating spike protein that is causing these adverse events. We have had constant debates for over a year now.
I apologise this article is a bit technical. Herein I demonstrate that circulating spike proteins can’t be the core root cause of the harm so many have suffered. Getting to the bottom of this is critical. Indeed many have been hurt exactly in the same way in the past with the same mechanism of harm but with different vaccines, with the same horrifying consequences …

A year after my father died, some forty years ago, his best friend kindly invited me with his family on a sailing cruise in Brittany. One day we ended up lost in the deepest fog I had ever seen. No wind to power our sails. Right in the middle of a very dense maritime route, off Saint Nazaire. These were pre-GPS days. Visibility was so low, one couldn’t see beyond a meter or two. Scary few hours. Without normal bearings, one’s brain starts imagining things. Trying to make sense of the unusual visual chaos, networks of neurones connect dots that have no connection. One starts seeing a dragon here, a huge cargo ship there …
That day, I learnt to triangulate radio signals emitted by land-based radio beacons. Getting a sense of location on a map comforted us. We couldn’t see the coastline or dangerous reefs, but we knew they were afar. We just hoped cargos would spot our radar reflector… The fog eventually faded away and all came back to normal, thankfully untouched and safe, with a clear view on the world.
It is time we get a clear view of the real damage vaccines - when not properly injected - have inflicted to the world. It is time to lift the fog stopping us from seeing the pervasiveness of bolus-induced vaccine injuries. Many have been asking me: “Why are you so persistent on investigating COVID vaccination? And why are you so insistent on your Bolus Theory1? We simply need to stop this. It’s the worse vaccines ever…”
Beyond the sad reality that as many as 644 million people2 might have been injured these past 2 years, and they are owed the truth, I have come to realise that past vaccination campaigns have also hurt billions of people.
For decades, we just didn’t see the accidents in the fog of our every day lives:
the distributed nature of vaccination :
across the age pyramid
spread evenly throughout the year
across vaccine technologies with varying degrees of harm
makes it impossible to relate harm to a possible injection accident.
the religious trust doctors and nurses have:
in the innocuity and the effectiveness of vaccines for decades
in their own pristine professionalism and absolute non-responsibility
in other reassuring causal relations: bed suffocation to explain SIDS, genetics for cancer, age for some disorders, etc …
make the very idea of vaccine-related harm absolutely impossible for the medical community to accept or even identify.
on top, safer vaccines - such as the traditional flu vaccines - have inevitably diluted the more severe adverse events that have happened.
For all these reasons and many others, it is quite evident that pharmaco-vigilance databases are, and have been, vastly under-reported. Even an illness tightly-associated with vaccine injuries such as Guillain-Barré only reported 4,399 in 32 years in VAERS for the entire US when GBS strikes 3000-6000 people every year in the US. An under-reporting of at least 26x, possibly as high as 52x. I only found 76 Alzheimer Disease reports in VAERS, when 500, 000 Americans are diagnosed every year! As explained in “Poking Holes in the Brain-Blood Barrier. Is that such a good idea?”, Alzheimer’s disease is necessarily correlated with vaccine bolus-induced brain-blood barrier leakage. So we have missed - and are missing - the vast majority of vaccine accidents.

The more we vaccinate, the more accidental intravascular injections occur, the more injuries trigger life-long diseases and deaths.

Come to think of it, in the statistics, these fateful accidents are now considered normal background noise, inexplicable, but normal. Collectively, we have come to accept the inacceptable as a part of life. I am certainly not stating these events are always injection-related, but I am more and more convinced they necessarily account for a very significant portion of these illnesses and deaths.
If we won’t get to the bottom of this perpetual under-the-surface disaster, people will continue to get hurt, and distrust to public health and the medical world will only amplify. As a community, we cannot afford not to learn from this vaccine crisis. This cycle of harm needs to end now!
And so, mistakenly scapegoating the “Circulating Spike” would be like sweeping all this harm and pain under the carpet. That’s intolerable.
Why Circulating Spikes Can’t be the Root Cause of COVID Vaccine Adverse Events
Time has come to look at the facts: There is no way the Circulating Spike can be the cause of the adverse Events that have been happening these past 2 years. One single falsifiable hypothesis is usually enough. Here I underline 12 different pieces of evidence. Too many falsifiable hypotheses prove it’s not possible that the circulating spike is responsible. Too many clinical signs point elsewhere. Too many studies also. Let me run you through how I got to that conclusion.
Hypothesis #1 - The Circulating Spike Hypothesis Breaks the Immunological Law of Antibody Neutralisation
If circulating spike are the root cause of the COVID-vaccines adverse events, it necessarily means either the antibodies were incapacitated or spike proteins escape antibodies roaming and neutralisation.
We know that billions of vaccinated people have produced spike proteins and antibodies. Multiple studies have shown spike clearance (most photos of spike staining show intracellular or intra-exosome spike, I have yet to see one with tissue stained).
The vast majority of vaccinated have had no adverse events. As expected by the Laws of Immunology, Antibody neutralisation has been proven to be effective. And there is no reason to believe that Antibody binding has become not functional, or has been incapacitated by the spike protein in any way.
This is a falsifiable hypothesis: Antibody neutralisation stands. Circulating spike protein as the root cause is invalidated.

Hypothesis #2 The Circulating Spike Hypothesis Breaks the Immunological Law of T-cell Priming and T-cell effectiveness
If circulating spike toxicity is the root cause of COVID-vaccine adverse events, notably from jab 2 onwards, that necessarily would mean that Spike-targeting T-cells would be letting transfected cells produce spike in large quantities despite prior priming by natural infection or via the first jab.
If circulating spikes are the root cause for these accidents, then that would be despite the Law of Immunology that states that once primed T-cells rapidly destroy all infected cells would be invalidated. And many studies have demonstrated anti-Spike T-cell are effective.
This is a falsifiable hypothesis: Law of T-cell Priming and T-cell effectiveness stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #2bis - Breaking the Immunological Law of T-cell Priming and T-cell effectiveness
Moreover, if not previously infected, a vaccinated should theoretically produce more spike proteins at the first injection than at the second or third injection (as confirmed in the chart below). So if spike production is inevitably more limited after jab 2, how is that compatible with AEs at injection 2 and more?
If the circulating spikes hypothesis is to be validated, Adverse Events (AE) should be principally happening after the first injection. And that is clearly not the case.
This is a falsifiable hypothesis: Law of T-cell Priming and T-cell effectiveness stands. Circulating spike protein as the root cause is invalidated.
In Toxicology, the Law of Threshold Toxicity of Poison states that below a certain threshold poison can be totally harmless, and only past a certain concentration or dose is the harm progressively becoming more severe.

Hypothesis #3 - The Circulating Spike Hypothesis Breaks the Law of Threshold Toxicity of Poisons
If effectively, the circulating spike is poisonous, then there should be a clear correlation in synchronicity between increase in dose/concentration of the poison in the plasma and accidents.
There is no synchronicity of Adverse Events with higher concentration of vaccinal spike in the blood. Several studies on circulating spike quantification (see above) have shown that Day 5 post-injection is the time when most spike proteins are circulating in the body. Adverse events have been shown to happen very quickly - deaths within 7 minutes - and often very late - 5 months after the date of vaccination. If the Spike protein is indeed found in the body in sufficient quantity to be a poison, then most accidents should be happening Day 5-6. This is not at all what we are witnessing, indicating, if not proving, that the spike isn't in large enough quantities to be poisonous, and once again disproving the hypothesis it is the circulating spike that is toxic.
This is a falsifiable hypothesis: Threshold Toxicity of Poisons stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #3bis - The Circulating Spike Hypothesis Breaks the Law of Threshold Toxicity of Poisons (amended for correction - mea culpa - the overwhelming antibody binding potential doesn't change anything to this hypothesis)
If effectively, the circulating spike is poisonous, then there should be a very significant amount of spike proteins presented in the blood to endothelial cells to compensate the wide antibody presence that was demonstrated.
Ogata et al have found a maximum of 150 picogram/mL on Day 5 which translates to 9 spike proteins in front of each endothelial cell at any given time, clearly not a convincing saturation level, when you have 13,000 antibodies "goal keeping" in front of each endothelial cell. This number overwhelms the binding capacity of a cell.
Even 1,000 fold increase in concentration gets the antibody capacity is 15 to 1
Only with a 10,000 times higher concentration (I don't see how Harvard could be soooo wrong!) could a saturation level possibly occur, and even then ACE-2 to antibody ratio is tiny, and so the 4,100 spike potentially binding would effectively be likely limited to less than 30.
This is a falsifiable hypothesis: Threshold Toxicity of Poisons stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #3ter - The Circulating Spike Hypothesis Breaks the Law of Threshold Toxicity of Poisons
If effectively, the circulating spike is poisonous, then the poison necessarily should trigger the same chemical and biological reactions in everyone.
Indeed some people previously infected might have an antidote (those are normally called antibodies) that should make them less prone to poisoning. Unfortunately, people exposed to the virus prior to vaccination have been shown to have more severe reactions to the vaccine (see below). This is incompatible with the spike being a poison. The more neutralised, the more poisonous doesn't make any sense.
This would tend to point more to the immune system being in cause.
This is a falsifiable hypothesis: Threshold Toxicity of Poisons stands. Circulating spike protein as the root cause is invalidated.

Hypothesis #3quater - The Circulating Spike Hypothesis Breaks the Law of Threshold Toxicity of Poisons
If effectively circulating spikes were poisonous, then the area of injection - where the highest transfection presumably occurs - and thus the most poisonous dose of Spike would inevitably be produced in a concentrated way should be the area of the body where a majority of adverse events occur, notably with serious necrosis similar to a snake bit.
There is no mention of Deltoid necrosis events in VAERS. The only adverse events related to the deltoid that I have read about is local pain. In other words, the place where there's the highest probability of poison presence is the place where there's no adverse event.
This is a falsifiable hypothesis: Threshold Toxicity of Poisons stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #3quinques - The Circulating Spike Hypothesis Breaks the Law of Threshold Toxicity of Poisons
If effectively, the circulating spikes were poisonous, then the infection fatality rate of SARS-COV-2 would necessarily be much higher than the flu or other common cold. A recent study from Stanford University demonstrated that the median IFR of SARS-COV-2 is 0.095% for the 0-69 years old. This underlines the fact that in the quantities of a viral infection (one would hope that the vaccine dose is lower) SARS-COV-2 is not particularly lethal. Therefore it is dubious that the vaccine would generate doses significant enough to be toxic.
This is a falsifiable hypothesis: Threshold Toxicity of Poisons stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #4 - The Circulating Spike Hypothesis Breaks the Law of Vascular Homogeneous Distribution
The human vascular system can be relied upon to constantly distribute evenly across the body all the chemical elements necessary for survival. If the circulating spike proteins are the root cause of the vaccine advert events, the spike proteins will evidently be spread homogeneously across the body, and necessarily be transported in the tissues.
Autopsies and pharmaco-vigilance data have demonstrated that the accidents are essentially localised on endothelial walls, the lining of the vascular system. This is utterly incompatible with a normal distribution of spike proteins throughout the body which would inevitably distribute spikes in the tissues. If the spike is indeed being integrated in large quantities via the ACE-2 receptors. There is no reason that would occur only on the endothelium.
This is a falsifiable hypothesis: The Law of Vascular Homogeneous Distribution stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #4bis - The Circulating Spike Hypothesis Breaks the Law of Vascular Homogeneous Distribution
As aforementioned, the human vascular system distributes homogeneously day-in day-out. However autopsies have systematically shown severe immune attacks in the arteries, and not in the veins.
As shown with the accumulation of clots in the veins, likely tied to autoimmune damage in the arteries, coagulation factor is transported down to the veinous system. If spike proteins were to accumulate and cause inflammation, it would likely be downstream from the arteries. It's a pharmaco-dynamic impossibility that it would accumulate in the aorta for example. Given the blood flow and pressure in the arteries, probabilities for spike accumulation would necessarily be either in the veins, or in the tissues. Factually, pathologists have observed immune-related damage occurs systematically in the arterial system.
This is a falsifiable hypothesis: The Law of Vascular Homogeneous Distribution stands. Circulating spike protein as the root cause is invalidated.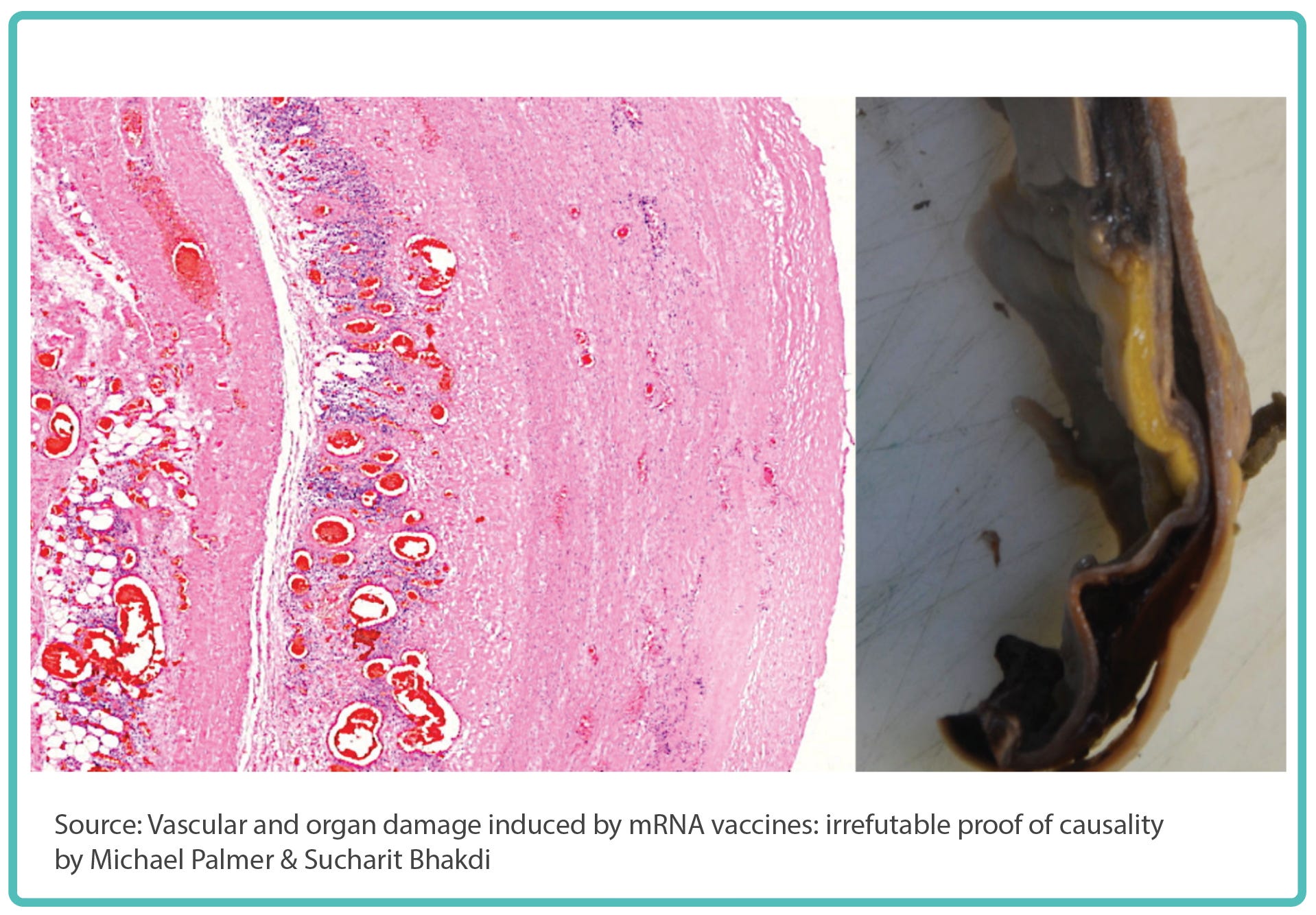
Hypothesis #4ter - The Circulating Spike Hypothesis Breaks the Law of Vascular Homogeneous Distribution
As witnessed when viruses become systemic in a body, the immune system attacks everywhere kickstarting cytokine storms. If the spike became systemic in very high concentrations, it is likely that cytokine storms would occur, and all organs would be failing simultaneously.
Severe adverse events related to COVID-vaccine injections are essentially localised, and mostly not systemic. On the contrary, many autopsies have uncovered concentrated immune attacks of the endothelium that are utterly incompatible with system-wide vascular system dissemination. Only a bolus injection could trigger such a discontinuity in vascular distribution.
This is a falsifiable hypothesis: The Law of Vascular Homogeneous Distribution stands. Circulating spike protein as the root cause is invalidated.
Hypothesis #4quintes - The Circulating Spike Hypothesis Breaks the Law of Vascular Homogeneous Distribution
The vascular system needs to deliver homogeneously not only in space, but also in time, as such only a fraction of the blood nutrients are delivered to the tissues at an instant (t), else the body would be depleted of fuel at a later stage. And so the vascular system is in fact an energy buffer, a form of fuel tank for the body.
And indeed, when I calculated where most of the spike is stored, 99.9% is stored in the center of the blood vessels, away from the endothelium. Only in the smallest capillary does this drop to 99%...This is the same logic that pharmaco-dynamic experts fight against when they want to deliver a drug to an organ. They need to bypass the systemic balance of vascular system.
This is a falsifiable hypothesis: The Law of Vascular Homogeneous Distribution stands. Circulating spike protein as the root cause is invalidated.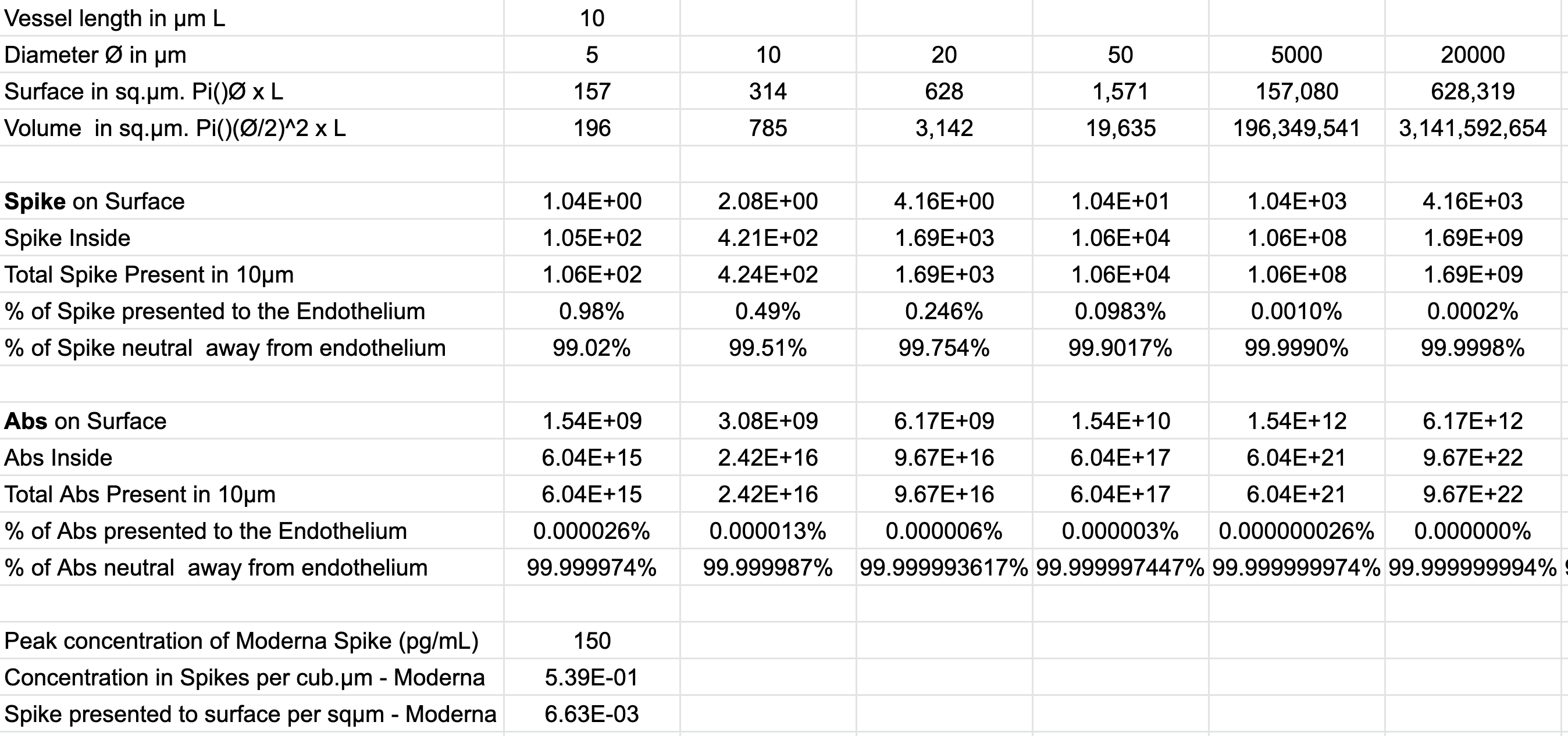
Evidently the Spike plays a key pathogenic role in the cells. Once nanoparticles have been up-taken by endothelial cells, these cells start producing spike which triggers a cytotoxic reaction. This is at the heart of the adverse events.
But I do not see how one can still believe that circulating spikes could be the underlying cause of adverse events. As I have detailed out, hopefully not to boringly, this assumption goes against robust laws of immunology and pharmacodynamics. The assumption is fundamentally flawed in at least 12 different ways, and goes against observable clinical data.
I know people who have become religious about the spike won’t change their minds in front of scientific proofs, but the evidence is clear the mechanism of harm of these vaccine is elsewhere…


The “Bolus Theory” is a theory I have developed whereby the combination of (1) a cytotoxic effect (kills cells) of a vaccine with (2) a direct accidental injection in the vascular system and (3) a rapid push of the seringue plunger, triggers a cascade of deleterious events in the body tied to the concentrated take up of vaccine particles by the endothelium leading to (A) arterial ruptures, (B) Vein thrombosis, (C) Organ inflammation, necrosis and failure, and (D) blood-tissue barrier leakage leading to a variety of illnesses (Sterility, Alzheimer’s…)
My estimation of accidental IV injection is 5% . 12.88 billion doses were injected to date. So one can estimate up to 644 million people could have been injured to a degree or another by the COVID vaccination campaigns. China’s procedure is unclear, and could lower that number 472 million.
Not really, 50 years ago people injecting did aspirate. Someone stupid decided to change that and nobody cared... 20 or 30 years ago.
Marc:
A couple comments of your article.
1. I acknowledge that we were raised differently. I am 73 years old and my father believed MDs were quacks. He often said that their "medicine" was "drugs and knives." (By "knives" he meant surgery.) He said the pillars of health were eating good food, exercising, getting adequate sleep, trying not to worry, getting outdoors for some sunshine and staying as far away from MDs as possible. I doubt that he ever heard the words "anti-vaxxer" but he was indeed an anti-vaxxer. He believed in trying to support your immune system by healthy living and not allowing someone to inject you with a concoction made in a laboratory. So, I admittedly recoil at your position that the issue is not the vaccines, but simply how they are administered.
2. However, I do believe that following the advice of the CDC to not aspirate is crazy. I believe that those who had an almost immediate metallic taste in their mouth had been injected intravenously. Nevertheless, I believe that these vaccines, like all vaccines, are harmful to some people. It is not just how they are administered; it is their bodies reaction to the actual vaccines.